![[exit]](/exit-outline.svg "Leave")
Details
This page contains information about POTS (Postural Orthostatic Tachycardia Syndrome) and potential therapies.
POTS has become a much more common occurance due to the prevalance of long covid since 2020 [1] and therefore it has become a larger focus of research, as it effects more of the population.
There are three types of POTS, including Hypovolemic POTS, Hyperadrenergic POTS and Neuropathic POTS.
POTS is commonly diagnosed based on a significant heart rate increase on standing from laying down (>30 bpm). While there are some potential therapies for POTS, there is no widely accepted option for those with POTS, and research is pretty limited. That being said, there are some options which may have potential for those with the condition.
Non-Pharmacological Therapies 
Derived from: [2].
- Fluid intake of at least 2.5L per day (Increases plasma volume)
- Salt (sodium chloride) intake of at least 9 grams per day (Increases fluid retention and plasma volume)
- Electrolyte Intake (Magnesium and Potassium)
- Compression stockings, waist high (Improves venous return)
- Vagus Nerve Stimulation (e.g with Pulsetto or Vielight Vagus) [6]
- Light exercise, such as swimming or recumbent bike (Potentially with CHOP protocol)
- Wedge mattress/pillow for sleeping & reclining chairs
- Smaller more frequent meals
General supplementation with needed vitamins is also recommended such as taking Iron, Vitamin B12, Vitamin D and others.
It is also recommended to avoid alcohol and most BP modulators.
Pharmacological Therapies
Potential treatments:
- Roxadustat (?) - Based on [5]
- Khavison Peptide Bioregulators (Ventfort, Cheloheart, Thylamin, Vladonix etc. ?)
- Tropisetron / Ondansetron (Anti-Nausea)
- Propranolol
- Ivabradine (Decreases heart rate)
- Mestinon (?)
- Low Dose ML-7 (Experimental)
Physiological Targets
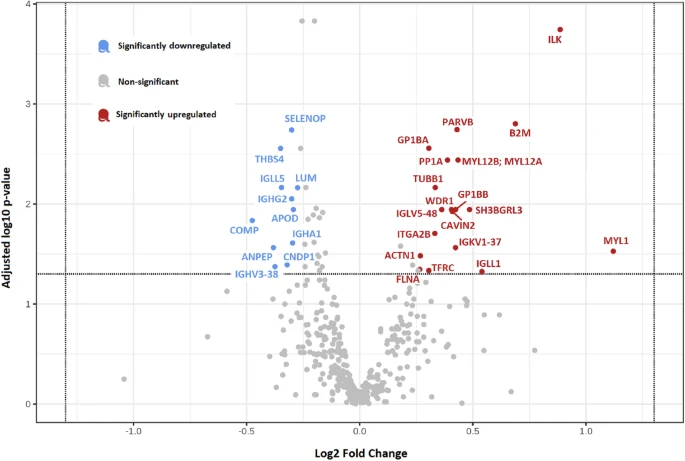
For upregulated alpha-adrenergic activity in POTS, MYL12B may be a target:
We noted significant upregulation of myosin regulatory light chain 12B (MYL12B) protein in POTS, which triggers polymerization of vascular smooth muscle. In POTS, increased sympathetic activation causes activation of the adrenergic receptors and a surge in norepinephrine levels, and approximately 89% of patients with POTS exhibit elevated levels of autoantibodies against the adrenergic α1 receptor. [3]
One potential approach for attenuation is through MYL12A/B inhibition. A compound by the name ML-7 may be a potential candidate. ML-7, for example inhibits proplatelet formation and stabilization [4], which is notably upregulated in POTS [3] ("Our study identified novel proteomic footprints in POTS linked to increased platelet activity").
Chronic Fatigue Relation
CFS is a common co-morbidity of POTS. It has been estimated that at least 21% of POTS patients have concurrent CFS.